

The Arrhythmic Substrate for Atrial Fibrillation in Patients with Mitral Regurgitation
- PMID: 34950292
- PMCID: PMC8691304
- DOI: 10.4022/jafib.2304
The Arrhythmic Substrate for Atrial Fibrillation in Patients with Mitral Regurgitation
Abstract
Objective: Patients with severe mitral regurgitation commonly develop atrial fibrillation. The precise mechanisms of this relationship remain unknown. The objective of this study was to apply noninvasive electrocardiographic imaging of the atria during sinus rhythm to identify changes in atrial electrophysiology that may contribute to development of atrial fibrillation in patients with severe mitral regurgitation referred for mitral valve surgery.
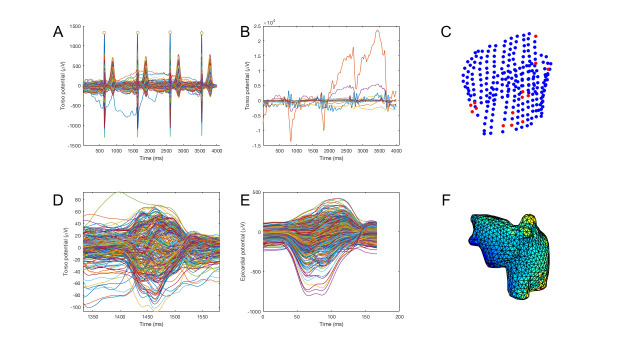
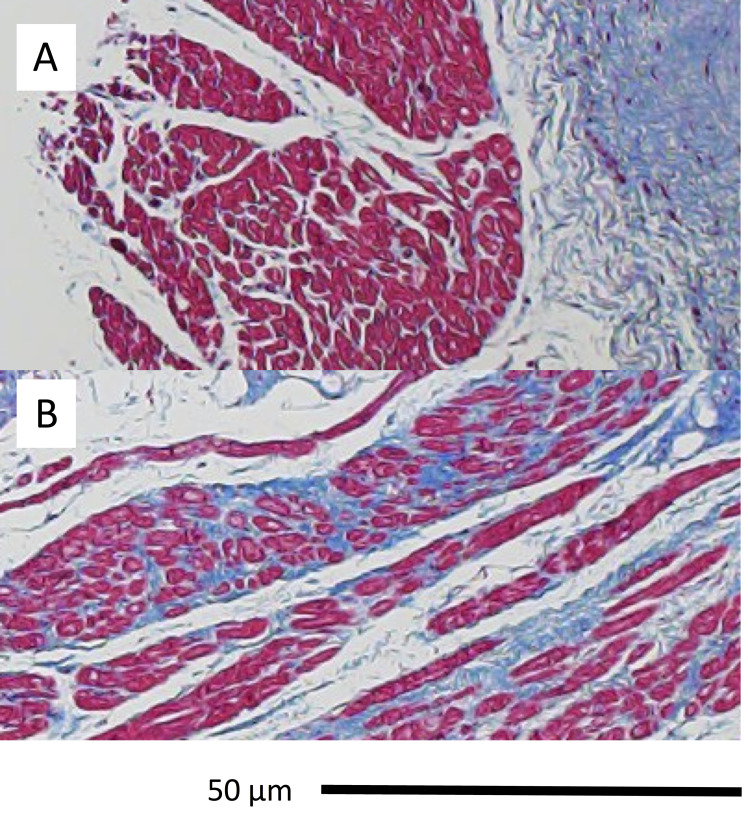
Methods: Twenty subjects (9 atrial fibrillation and mitral regurgitation, 11 mitral regurgitation alone) underwent electrocardiographic imaging. Biatrial electrophysiology was imaged with activation maps in sinus rhythm. The reconstructed unipolar electrograms were analyzed for voltage amplitude, number of deflections and conduction heterogeneity. In subjects with mitral regurgitation, left atrial biopsies were obtained at the time of surgery. Results: Subjects with history of atrial fibrillation demonstrated prolonged left atrial conduction times (110±25 ms vs. mitral regurgitation alone (85±21), p=0.025); right atrial conduction times were unaffected. Variable patterns of conduction slowing were imaged in the left atria of most subjects, but those with prior history of atrial fibrillation had more complex patterns of conduction slowing or unidirectional block. The presence of atrial fibrillation was not associated with the extent of fibrosis in atrial biopsies.
Conclusions: Detailed changes in sinus rhythm atrial electrophysiology can be imaged noninvasively and can be used to assess the impact and evolution of atrial fibrillation on atrial conduction properties in patients with mitral regurgitation. If replicated in larger studies, electrocardiographic imaging may identify patients with mitral regurgitation at risk for atrial fibrillation and could be used to guide treatment strategies.
Keywords: Atrial Fibrillation; Electrocardiographic Imaging; Inferior Vena Cava.
Figures


Similar articles
-
Mitochondrial apoptotic pathway activation in the atria of heart failure patients due to mitral and tricuspid regurgitation.Exp Mol Pathol. 2015 Aug;99(1):65-73. doi: 10.1016/j.yexmp.2015.05.007. Epub 2015 May 22. Exp Mol Pathol. 2015. PMID: 26004742
-
Electrophysiological properties in patients undergoing atrial compartment operation for chronic atrial fibrillation with mitral valve disease.Eur Heart J. 1997 Nov;18(11):1805-15. doi: 10.1093/oxfordjournals.eurheartj.a015176. Eur Heart J. 1997. PMID: 9402456
-
Outcome of mitral valve repair in patients with preoperative atrial fibrillation. Should the maze procedure be combined with mitral valvuloplasty?J Thorac Cardiovasc Surg. 1994 Feb;107(2):408-15. J Thorac Cardiovasc Surg. 1994. PMID: 8302059
-
Looking into the Mechanistic Link Between Mitral Regurgitation and Atrial Fibrillation.Cardiol Clin. 2021 May;39(2):281-288. doi: 10.1016/j.ccl.2021.01.010. Epub 2021 Mar 23. Cardiol Clin. 2021. PMID: 33894941 Review.
-
Mechanistic insights into mitral regurgitation due to atrial fibrillation: "Atrial functional mitral regurgitation".Trends Cardiovasc Med. 2016 Nov;26(8):681-689. doi: 10.1016/j.tcm.2016.04.012. Epub 2016 May 2. Trends Cardiovasc Med. 2016. PMID: 27345155 Review.
Cited by
-
Electrocardiographic imaging in the atria.Med Biol Eng Comput. 2023 Apr;61(4):879-896. doi: 10.1007/s11517-022-02709-7. Epub 2022 Nov 12. Med Biol Eng Comput. 2023. PMID: 36370321 Free PMC article. Review.
-
Electrocardiographic Imaging for Atrial Fibrillation: A Perspective From Computer Models and Animal Experiments to Clinical Value.Front Physiol. 2021 Apr 30;12:653013. doi: 10.3389/fphys.2021.653013. eCollection 2021. Front Physiol. 2021. PMID: 33995122 Free PMC article. Review.
References
-
- Lim E, Barlow C W, Hosseinpour A R, Wisbey C, Wilson K, Pidgeon W, Charman S, Barlow J B, Wells F C. Influence of atrial fibrillation on outcome following mitral valve repair. Circulation. 2001 Sep 18;104 (12 Suppl 1):I59–63. - PubMed
-
- Chiang Chern-En, Naditch-Brûlé Lisa, Murin Jan, Goethals Marnix, Inoue Hiroshi, O'Neill James, Silva-Cardoso Jose, Zharinov Oleg, Gamra Habib, Alam Samir, Ponikowski Piotr, Lewalter Thorsten, Rosenqvist Mårten, Steg Philippe Gabriel. Distribution and risk profile of paroxysmal, persistent, and permanent atrial fibrillation in routine clinical practice: insight from the real-life global survey evaluating patients with atrial fibrillation international registry. Circ Arrhythm Electrophysiol. 2012 Aug 01;5 (4):632–9. - PubMed
-
- Nkomo Vuyisile T, Gardin Julius M, Skelton Thomas N, Gottdiener John S, Scott Christopher G, Enriquez-Sarano Maurice. Burden of valvular heart diseases: a population-based study. Lancet. 2006 Sep 16;368 (9540):1005–11. - PubMed
-
- Grigioni Francesco, Avierinos Jean-François, Ling Lieng H, Scott Christopher G, Bailey Kent R, Tajik A Jamil, Frye Robert L, Enriquez-Sarano Maurice. Atrial fibrillation complicating the course of degenerative mitral regurgitation: determinants and long-term outcome. J Am Coll Cardiol. 2002 Jul 03;40 (1):84–92. - PubMed
-
- Nishimura Rick A, Otto Catherine M, Bonow Robert O, Carabello Blase A, Erwin John P, Fleisher Lee A, Jneid Hani, Mack Michael J, McLeod Christopher J, O'Gara Patrick T, Rigolin Vera H, Sundt Thoralf M, Thompson Annemarie. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017 Jun 20;135 (25):e1159–e1195. - PubMed